Clinical information
Alzheimer’s disease (AD) is the most common cause of dementia in old age, accounting for 60 % to 70 % of cases. The prevalence doubles about every five years from the age of 65, meaning that 30 % of people over the age of 90 have AD. The disease is characterised by a progressive and irreversible decline in cognitive abilities. The disease course is divided into three consecutive phases: the preclinical stage, the MCI (mild cognitive impairment) stage and the dementia stage. In AD, protein deposits associated with the destruction of nerve cells form in the brain.
Neurofibrillary tangles made up of hyperphosphorylated tau protein (pTau(181)) accumulate in the nerve cells (particularly in the cortical and limbic regions of the brain). Tau is expressed in neurons to stabilise the microtubules of the cytoskeleton. Impaired phosphorylation of this protein leads to aggregation in the form of neurofibrils, which accumulate in the bodies of nerve cells and disrupt the axonal transport.
Accumulations of senile plaques, consisting mainly of beta-amyloids (Aβ), can be found outside the nerve cells. These are peptides formed by the processing of the membrane-spanning amyloid precursor protein (APP), of which there are several isoforms. In AD, the breakdown of these peptides is impaired, leading to plaque deposits, particularly made up of beta-amyloid (1-40) (Aβ1-40) and beta-amyloid (1-42) (Aβ1-42).
In recent years, one focus of AD research has been on the development of monoclonal antibodies (mAbs) that are directed against Aβ plaques and thus enable treatment of the disease. However, clinical studies have shown that treatment with anti-Aβ antibodies can have a side effect called amyloid-related imaging abnormalities (ARIA), which can be life-threatening. The risk of developing ARIA with anti-Aβ antibody treatment varies depending on the genotype of the apolipoprotein E (APoE) gene that a patient carries, so genotyping is useful in assessing this risk.
Diagnostics
 A definitive diagnosis of AD can only be made by histological examination of a sample of brain tissue from the deceased patient (detection of plaques and neurofibrillary tangles). In living patients, AD can only be diagnosed as probable. This is based on clinical recognition of the dementia syndrome and exclusion of possible reversible causes. Positron emission tomography (PET) can provide further information, as it is now also possible to visualise the specific neuropathological changes in living patients. The determination of biomarkers in cerebrospinal fluid (CSF) has also become an established part of Alzheimer’s diagnostics. These can also indicate the disease with a high degree of certainty.
A definitive diagnosis of AD can only be made by histological examination of a sample of brain tissue from the deceased patient (detection of plaques and neurofibrillary tangles). In living patients, AD can only be diagnosed as probable. This is based on clinical recognition of the dementia syndrome and exclusion of possible reversible causes. Positron emission tomography (PET) can provide further information, as it is now also possible to visualise the specific neuropathological changes in living patients. The determination of biomarkers in cerebrospinal fluid (CSF) has also become an established part of Alzheimer’s diagnostics. These can also indicate the disease with a high degree of certainty.
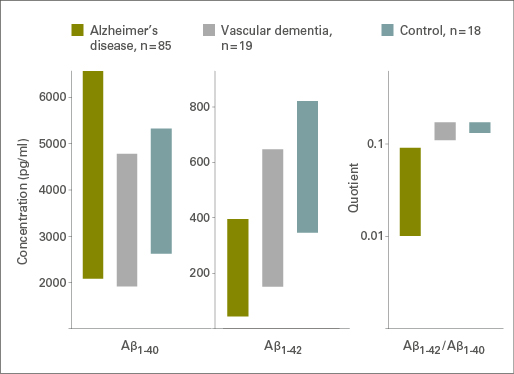
CSF samples from persons who will develop AD show a significant decrease in the Aβ1-42 levels already 5 to 10 years before the onset of cognitive changes. In contrast, the concentrations of total tau and pTau(181) increase when patients show advanced neurodegeneration and cognitive impairment. Furthermore, the amyloid ratio Aβ1-42/Aβ1-40 may help to differentiate AD from vascular dementia (see figure). The calculation of the ratio also reduces the confounding influence of preclinical factors on the measured concentrations.
The results from the CSF-based neurochemical analyses should only be interpreted in the context of all available diagnostic information.
Did we spark your interest? Find out more about APOE genotyping and EUROIMMUN’s test portfolio!
Files
Diagnosing Alzheimer’s disease - A new generation of tests from EUROIMMUN
 Preanalytics in dementia diagnostics
Preanalytics in dementia diagnostics
Recognising external impact factors and optimising procedures
more information




















