EUROLINE
positive control serum: IgG, human, 100x concentrated
for DL 1300-X G
EUROASSAY
AMA M2, LKM-1, SLA/LP
EUROASSAY strip
with antigens
IIFT
Liver Mosaic 1
liver-kidney microsomes (LKM), ANA
mitochondria (AMA), LKM
2 BIOCHIPs per field:
liver
kidney
rat
rat
EUROLINE
Liver Profile 2
(AMA M2, M2-3E, LKM-1, LC-1, SLA/LP separately)
EUROLINE
IIFT
Liver Screen 1
mitochondria (AMA), LKM
soluble liver antigen/
liver-pancreas antigen (SLA/LP)
LKM, ANA
smooth muscles (ASMA)
4 BIOCHIPs per field:
kidney
transfected cells
liver
stomach
rat
EU 90
rat
rat
EUROASSAY
Liver Profile
AMA M2, LKM-1, LC-1, SLA/LP
EUROASSAY strip
with antigens
EUROLINE
Liver Profile
(AMA M2, LKM-1, LC-1, SLA/LP separately)
EUROLINE
EUROLINE
Autoimmune Liver Diseases
(AMA M2, M2-3E, Sp100, PML, gp210,
LKM-1, LC-1, SLA/LP, Ro-52 separately)
EUROLINE
EUROLINE
Autoimmune Liver Diseases 14 Ag
(AMA-M2, M2-3E, Sp100, PML, gp210,
LKM-1, LC-1, SLA/LP, SS-A, Ro-52, Scl-70,
CENP A, CENP B, PGDH separately)
EUROLINE
IIFT
Liver Mosaic 8
liver antigens, cell nuclei (ANA)
F-actin
cell nuclei (ANA)
LKM, ANA
mitochondria (AMA), LKM
smooth muscles (ASMA)
6 BIOCHIPs per field:
liver
VSM47
HEp-2 cells
liver
kidney
stomach
monkey
rat
human
rat
rat
rat
EUROLINE
Autoimmune Liver Diseases 9 Ag plus F-Actin
(AMA-M2, M2-3E, Sp100, PML, gp210,
LKM-1, LC-1, SLA/LP, F-Aktin und Ro-52)
EUROLINE
IIFT
Autoimmune liver diseases Screen 9
EUROPattern
mitochondria (AMA), LKM
LKM, ANA
smooth muscles (ASMA)
F-actin
4 BIOCHIPs per field:
kidney
liver
stomach
VSM47
rat
rat
rat
rat
IIFT
Liver Mosaic 9
mitochondria (AMA), LKM
LKM, ANA
smooth muscles (ASMA)
F-actin
4 BIOCHIPs per field:
kidney
liver
stomach
VSM47
rat
rat
rat
rat
EUROASSAY
SLA/LP
EUROASSAY strip
with antigens
ELISA
soluble liver antigen/
liver-pancreas antigen (SLA/LP)
antigen-coated
microplate wells
IIFT
soluble liver antigen/
liver-pancreas antigen (SLA/LP)
transfected cells
control transfection
(2 BIOCHIPs per field)
EU 90
EU 90
ELISA
cytosolic
liver antigen type 1
(LC-1)
antigen-coated
microplate wells
IIFT
antibodies against liver-kidney microsomes
(LKM ab control)
ChLIA
IDS Liver Control Set
1
3 x 1.0 ml Control 1/2
ChLIA
IDS LKM-1 1
antigenic coated magnetic particles
ELISA
liver-kidney microsomes
(LKM-1)
antigen-coated
microplate wells
IIFT
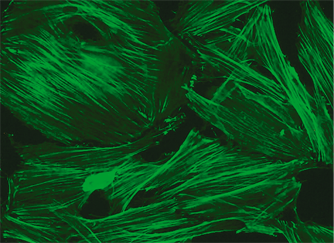
antibodies against F-actin
IIFT
F-actin EUROPattern
VSM47
rat
IIFT
antibodies against smooth muscles
(ASMA control)
IIFT
smooth muscles
(ASMA)
stomach
rat
IIFT
smooth muscles (ASMA)
F-actin
stomach
VSM47
(2 BIOCHIPs per field)
rat
rat
IIFT
Mosaic Basic Profile 1
cell nuclei (ANA)
mitochondria (AMA)
smooth muscles (ASMA)
3 BIOCHIPs per field:
HEp-2 cells
kidney
stomach
human
rat
rat
IIFT
Mosaic Basic Profile 2 EUROPattern
cell nuclei (ANA), LKM
mitochondria (AMA), LKM
smooth muscles (ASMA)
3 BIOCHIPs per field:
liver
kidney
stomach
rat
rat
rat
IIFT
Mosaic Basic Profile 2
cell nuclei (ANA), LKM
mitochondria (AMA), LKM
smooth muscles (ASMA)
3 BIOCHIPs per field:
liver
kidney
stomach
rat
rat
rat
IIFT
Mosaic Basic Profile 3
cell nuclei (ANA)
cell nuclei (ANA)
mitochondria (AMA)
smooth muscles (ASMA)
4 BIOCHIPs per field:
HEp-2 cells
liver
kidney
stomach
human
monkey
rat
rat
IIFT
Mosaic Basic Profile 3A EUROPattern
cell nuclei (ANA) EUROPattern
cell nuclei (ANA)
mitochondria (AMA)
smooth muscles (ASMA)
4 BIOCHIPs per field:
HEp-20-10 cells
liver
kidney
stomach
human
monkey
rat
rat
IIFT
Mosaic Basic Profile 3A
cell nuclei (ANA)
cell nuclei (ANA)
mitochondria (AMA)
smooth muscles (ASMA)
4 BIOCHIPs per field:
HEp-20-10 cells
liver
kidney
stomach
human
monkey
rat
rat
IIFT
Mosaic Basic Profile 3C EUROPattern
cell nuclei (ANA), EUROPattern
cell nuclei (ANA), LKM
mitochondria (AMA), LKM
smooth muscles (ASMA)
4 BIOCHIPs per field:
HEp-20-10 cells
liver
kidney
stomach
human
rat
rat
rat
IIFT
Mosaic Basic Profile 3C
cell nuclei (ANA)
cell nuclei (ANA), LKM
mitochondria (AMA), LKM
smooth muscles (ASMA)
4 BIOCHIPs per field:
HEp-20-10 cells
liver
kidney
stomach
human
rat
rat
rat




















 Circulating autoantibodies have come to play a significant role in the diagnosis of AIH. They occur in the majority of patients, although their role in the pathogenesis is still unclear. There is also no clear correlation between the disease activity or prognosis and the antibody titer.
Circulating autoantibodies have come to play a significant role in the diagnosis of AIH. They occur in the majority of patients, although their role in the pathogenesis is still unclear. There is also no clear correlation between the disease activity or prognosis and the antibody titer.